
There’s a lot going on in the luteal or premenstrual phase of the menstrual cycle, including higher histamine and an increased requirement for sodium. And if you’ve been struggling with hormonal mood symptoms, the solution might be simpler than you think.
Check out episode 19 of my podcast, where I explore the luteal phase.
🟦

Also available wherever you get your podcasts.
Transcript
Welcome back to the podcast. I’m your host, Lara Briden, a naturopathic doctor and author of the books Period Repair Manual, Hormone Repair Manual, and Metabolism Repair for Women.
I’m currently working on a new book about periods, so thinking a lot about the fact that female physiology is cyclic. Or we could say that human physiology is cyclic, except for men, who make their hormones in a quirky daily pattern. Everybody else, namely women, makes hormones approximately monthly.
And, of course, hormones impact all aspects of health, including metabolism, gut, immune activity, and, of course, the brain. Therefore, with cyclic physiology, we move through different gears, modes, or ways of doing things. That’s a normal part of being human.
First, there’s the early follicular, low-hormone state. That’s during or just after the bleed. Mood-wise, many women are on reasonably good terms with this low hormone mode. But not everyone, and we’ll come to that.
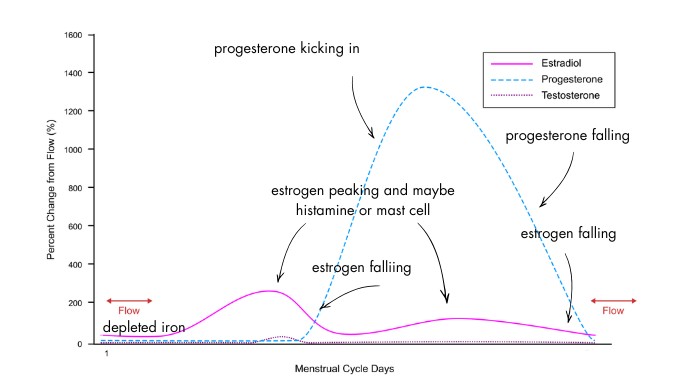
Next, estradiol or estrogen starts to ramp up on the way to ovulation, and most women feel pretty good with that. In fact, some women feel really good as both serotonin and dopamine rise with estrogen. That is, until estrogen starts to stimulate mast cells and histamine, which is a stimulating neurotransmitter. And we’ll come to that.
After ovulation, estrogen dips and progesterone kicks in. And that should feel okay, but it is a significant change. You’re swinging from the bubbly, outgoing follicular to the more inward or subdued start of the luteal. Progesterone is on the rise, but so is estrogen for its second peak. Again, most women feel pretty good at this time, although somewhat hungrier and sleepier.
Finally, there’s the late luteal, when both estrogen and progesterone take a nosedive. As your hormones make their final exit, it’s normal to feel something… which could be fatigue, or maybe more jittery or irritable. That’s the classic premenstrual picture.
And to be clear: All of that is with ovulatory cycles or cycles where you ovulate.
Anovulatory cycles are different. They are the cycles where you don’t ovulate, but still go on to bleed. Hormones look like this if you’re watching the video. Some ups and downs of estrogen, but no progesterone at all. Anovulatory cycles are fairly common. And the best way to know if you’re having one versus a proper ovulatory cycle is to track your basal body temperature or BBT, which rises in the luteal phase.
And of course, if you’re on birth control, especially an estrogen method like many pills, patches, or the NuvaRing, then you do not have a cycle. Your own ovarian hormones are close to flat-lined, and you really only make estradiol, in pink if you’re watching the video, when you take the non-active or sugar pills. In place of real hormones, you have the synthetic hormones of birth control. But, to be clear, the synthetic hormones of birth control are not estradiol and progesterone. And any mood problems on the pill are not a premenstrual or a luteal problem, but rather a side effect of the synthetic hormone. So, birth control doesn’t really come into this discussion.
Because today we’re talking about the luteal phase and why, for most women, it can feel different from the follicular phase. And why, for some women, it can feel absolutely terrible. That would be more in the territory of PMDD or premenstrual dysphoric disorder, which affects about one in 20 women. And if that’s your situation, you may still benefit from some natural approaches, but you should also be under the care of a specialist.
Okay, so for the milder version of premenstrual mood symptoms, what is up with the luteal phase? Is it just that progesterone makes you feel bad? Or, more logically, that losing it does? Because, in theory, progesterone should feel great thanks to its neurosteroid metabolite allopregnanolone that interacts with GABA receptors and normally calms them.
I say normally, because sometimes allopregnanolone can have a paradoxical, anxiety effect on GABA receptors. For more about that, see my blog post or article called “Why progesterone is both good and bad for mood.” And just a comment that the theory behind prescribing SSRIs for PMDD is not to increase serotonin, but rather to increase allopregnanolone, which is interesting and does raise the question of whether it would also be possible to just take progesterone. And sometimes it is.
For today, though, I want to move a little beyond the neurotransmitter discussion and think about the luteal phase as a whole-body transformation. A different mode or way of doing things that impacts physiology at almost every level.
So, yes, there are more tranquilising neurotransmitters around in the luteal. And why is that? Because your body is trying to slow down and prepare for a pregnancy. That’s why you need more sleep and rest in the luteal. That’s normal. You also need more food and nutrients of every kind, including protein, carbs, and sodium. And that’s because progesterone promotes the loss of sodium. So you could feel much better by just taking electrolytes, with a good dose of sodium. And, during the luteal, you also need more magnesium, which is why magnesium can be so, so helpful.
In the luteal phase, you’ll shift to mildly reduced insulin sensitivity. Again, that’s adaptive for a potential pregnancy. It’s an example of when mild insulin resistance can be normal or physiological, not pathological. However, if you’re not fully nourished, especially if you’re not getting enough protein, then that mild shift in insulin sensitivity could make you more vulnerable to drops in blood sugar, which can feel a lot like anxiety. For more on low blood sugar and how to treat it, check out episodes 15 and 16 of the podcast. And always remember that increased hunger in the luteal is not a dysfunction or a failure on your part. It’s simply how female physiology works. So, you need to eat more.
Next, the luteal phase involves some pretty complex immune changes, including the possibility of increased inflammation and pain, in part from things like increased intestinal permeability, but also from the rise of the hormone prolactin that can drive inflammation and pain. There’s a link in the show notes to some interesting research about prolactin and pain.
Another driver of inflammation at the end of the luteal is the loss of both estrogen and progesterone. Because the hormones have beneficial anti-inflammatory properties. Progesterone, in particular, is immune-modulating or anti-inflammatory in a way that can reduce the risk of autoimmunity or the autoimmune type of inflammation. And that’s why taking natural progesterone can often improve fibromyalgia-type pain and migraines.
Finally, as part of the immune changes, some women can experience mast cell activation and high histamine, contributing to symptoms like anxiety, agitation, and insomnia. That’s because histamine is a neurotransmitter. Also, nasal congestion, rash, breast pain, headaches, heavy menstrual flow, and, interestingly, relief from antihistamines or antihistamine strategies, which we’ll come to in a minute. That could almost be used diagnostically. So, if you improve with antihistamines, it suggests this is part of what’s going on.
If histamine is involved, hormonal symptoms will usually coincide with rising or peaking estrogen. And that’s because estrogen can increase histamine via various mechanisms, including the direct activation of mast cells. At the same time, in the other direction, histamine can increase estrogen. So, it becomes a vicious cycle or a perfect storm of high estrogen and high histamine. And to say again, that is most likely to happen with your estrogen peaks, which are just before ovulation, and then again mid-luteal. And that’s why body literacy is so important, which is knowing if and when you ovulate. So you can understand your symptoms in the context of the underlying hormonal events.
In terms of treatment, if you’re dealing with the high estrogen-high histamine type of symptoms, you want to think about reducing estrogen by maintaining a healthy gut, avoiding alcohol, and maybe taking iodine, which can have a beneficial anti-estrogen effect. Link in the show notes to my iodine article. You’ll also likely need an antihistamine approach, such as an over-the-counter antihistamine or a natural strategy like avoiding normal dairy or A1 casein, addressing any gut issues, antihistamine supplements like vitamin B6, SAM-e, or natural progesterone, and regulating the nervous system.
And, of course, regulating the nervous system is crucial for any aspect of health, especially mood symptoms.
Now, high histamine is one reason a tendency to higher estrogen can feel a little rough. Another is that the higher estrogen goes, the further it has to fall at the end of the cycle, just before the period. Because, remember, it’s normal for estrogen to drop to rock-bottom levels every cycle. The problem isn’t low estrogen, but rather falling estrogen, which can cause symptoms like night sweats, increased hunger, and migraines. Estrogen also drops a little just after ovulation, so that’s worth considering or watching for.
And, then, big picture, the end of the cycle is also when progesterone falls, and that means losing its GABA support, contributing to symptoms like anxiety and sleep disturbance. Treatments to support GABA include the classic premenstrual treatments like magnesium, taurine, glycine, B-complex, including vitamin B6, and herbal medicines like kava and passionflower. This is also when taking progesterone or body-identical progesterone can be very helpful, either as a cream or capsule. That’s potentially true even if you think you have progesterone sensitivity. Sometimes you just need to go higher with the dose, not lower. I discuss that in the “Why progesterone is both good and bad for mood” article I mentioned earlier.
And if symptoms continue into the period or maybe just after the period, that could be because estrogen is low then, which can, in some cases, be helped by supplementing estrogen. I discuss that in my books.
But during the period is also when iron can be low, depleted by the flow. So, make sure your iron is okay, especially if you have heavy flow. Ask your doctor to test iron studies, and your ferritin should be at least 50 micrograms per litre. That’s especially true for post-menstrual migraines or migraines right after the bleed.
Okay, so we’ve been looking at how to interpret hormonal symptoms based on when they occur relative to the different hormonal events of the cycle.
As a review, we’ve talked about the high histamine from the estrogen peaks. Then, the withdrawal from falling estrogen and progesterone at the end of the cycle. We touched on low estrogen and, probably more importantly, low or depleted iron early in the cycle, can be a factor.
Next, we need to consider symptoms that hit at the onset of the luteal, when progesterone kicks in. But before we get to that, I’ll just point out that prolactin is also higher in the luteal phase. Not dramatically higher like progesterone, but somewhat higher, and it can increase hunger, pain, and anxiety. There’s also an interesting dopamine connection in that a tendency to lower dopamine could mean higher prolactin. That’s because dopamine should normally push down on prolactin and keep it in check. And that’s probably why low dopamine states, like ADHD, have been linked to premenstrual mood symptoms—see the show notes for that research. And see my prolactin article for more about symptoms, testing, and treatment ideas, including the well-known and much-loved chaste tree or vitex, which can be a great treatment for PMS and has done well in several clinical trials.
Finally, thinking about progesterone kicking in, let’s circle back to how the luteal phase is a whole-body transformation. A big part of what’s going on is that progesterone asks a lot from you. It’s trying to prepare you for pregnancy, so your luteal mode needs more sleep, rest, and nourishment, including calories, protein, and all the nutrients, especially sodium and magnesium. And, big picture, if your body’s needs are not being met, your poor nervous system could understandably feel more fragile. And sometimes the solution is something as simple as resting more, eating more, or taking a simple electrolyte or mineral supplement. In that way, maybe the luteal phase is not so much a problem to be fixed, but more of an invitation or opportunity to give your body everything it needs.
Okay. I hope that’s been helpful, and thanks so much for listening! Or watching.
Please share and leave a review. You can also leave a comment on the YouTube video or the article/blog post associated with this episode at LaraBriden.com. And I’ll see you next time for a discussion of wheat sensitivity and how it can impact periods.