When it comes to mood, progesterone is a paradox.
For most women, it’s soothing, thanks to its calming effect on the brain. But for some, it can trigger anxiety, irritability, or even rage. What’s going on?
💡 Also read: Troubleshooting progesterone and Top 6 natural treatments for premenstrual mood symptoms
Progestins can be bad for mood, but they’re not progesterone
If you’ve had a negative reaction to hormonal birth control, especially “progesterone-only” methods, consider that those are progestins, not natural progesterone. Unfortunately, many doctors, journalists, and even scientists still confuse the two and mistakenly blame progesterone for progestins’ negative mood effects.
Common progestins include levonorgestrel, drospirenone, and norethisterone. Their impact on mood is a drug side effect, not premenstrual mood symptoms.
How progesterone affects the brain
Natural progesterone converts to allopregnanolone, a calming neurosteroid that interacts with GABA receptors.
That’s why:
- you might feel drowsy during the luteal phase,
- pregnancy can bring a sense of calm,
- progesterone capsules are sedating. and
- body-identical or natural progesterone usually improves mood.
Importantly, no progestins convert to allopregnanolone, so progestins cannot soothe mood like progesterone.
When progesterone feels bad: PMDD and the GABA receptor
For some women—including those with premenstrual dysphoric disorder (PMDD)—progesterone’s calming metabolite allopregnanolone does the opposite. Instead of soothing the brain, it agitates it.
That’s partly because allopregnanolone can have a “biphasic” or Goldilocks effect on GABA receptors:
- Low doses irritate GABA receptors and spark anxiety, especially when estrogen is high.
- Higher doses calm them.
Furthermore, there can be a problem with the flexibility or adaptability of GABA receptors, which are supposed to “reshuffle” their subunits and adapt to the dramatic ups and downs of allopregnanolone across the menstrual cycle.
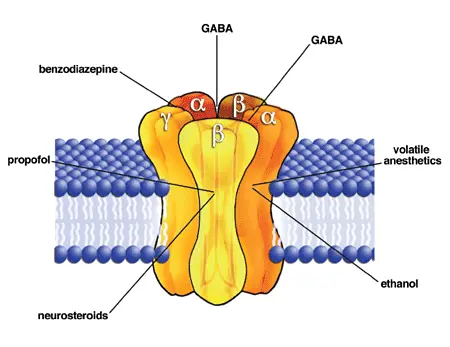
For some women, that adaptive flexibility can be impaired by factors such as inflammation, high histamine, or even genetics. For example, a 2025 Nature study found that women with PMDD have reduced expression of the δ subunit of the GABA-A receptor during the luteal phase, which contributes to higher reactivity of the amygdala, the brain’s emotion center.
Solutions include reducing inflammation and lowering histamine (see below), plus taking the right dose of progesterone.
How to take progesterone for premenstrual or perimenopuasal mood symptoms
Because of the biphasic GABA response, a higher nighttime dose of oral progesterone (300 mg) can sometimes work better than a lower dose—especially for severe premenstrual symptoms such as PMDD. And especially when estrogen is high.
For milder symptoms that appear at the end of the cycle (when progesterone drops), lower-dose progesterone (such as a cream) may be enough.
If you’ve ever had a negative mood reaction to progesterone, consider:
- Was it actually a progestin (synthetic), not progesterone? If so, body-identical could still be fine.
- If it was natural progesterone, you may still be able to tolerate it by 1) lowering inflammation, histamine, or estrogen, or 2) going up in dose, not down. But check with your clinician.
- Doses over 400 mg can knock you out—causing grogginess or even depression, especially if taken during the day.

Beyond progesterone and GABA
Of course, there’s more to premenstrual mood symptoms than GABA receptors. Other factors include:
- Gut inflammation and mast cell activation (histamine is a stimulating neurotransmitter that fluctuates across the cycle).
- Low sodium, since progesterone promotes sodium loss, and low sodium is linked to anxiety. That’s why salt or electrolytes can sometimes help.
Natural treatment for premenstrual mood symptoms
As I discuss in my PMDD podcast/YouTube video, other PMDD treatment strategies include:
- Reduce histamine and mast cell activation because histamine is a stimulating neurotransmitter linked to various mental health symptoms, including anxiety, and it fluctuates across the menstrual cycle. Lowering histamine can also help to stabilize GABA receptors.
💡Tip: A simple antihistamine can sometimes relieve mood symptoms.
💡Tip: Avoiding A1 cow’s dairy can help to prevent a mast cell or histamine reaction.
- Take magnesium to support a healthy GABA response and “normalize the action of progesterone on the central nervous system.” The best form is magnesium glycinate or bisglycinate because the amino acid glycine also calms GABA receptors. Consider taking a formula with taurine, because taurine also calms GABA receptors.
💡Tip: The therapeutic dose is 300 mg of elemental magnesium, so check the label. Most magnesium capsules provide only 100 mg.
- Add vitamin B6 (pyridoxine) to boost GABA, lower prolactin, and promote the healthy clearance of histamine. Be careful because too much B6 can cause nerve damage.
- Consider iodine, which is one of my favourite prescriptions for premenstrual mood symptoms and breast pain.
Share your experience!