Progesterone has anti-androgen benefits and can promote ovulation. That makes progesterone therapeutic for polycystic ovary syndrome, as described in my paper The central role of ovulatory disturbances in the etiology of androgenic polycystic ovary syndrome (PCOS)—Evidence for treatment with cyclic progesterone.
By progesterone, I mean real progesterone, also called body-identical progesterone or oral micronized progesterone (OMP), which is available in products such as Prometrium, Utrogestan, Teva, and Famenita, depending on your country. Progestins, on the other hand, are not progesterone and do not exert the same ovulation-promoting effect. And although some progestins (e.g. drospirenone) are anti-androgenic, others (e.g. levonorgestrel) are androgenic or testosterone-like and can worsen the androgen excess and insulin resistance of PCOS.
PCOS begins in the brain
Most evidence points to a “neuroendocrine” basis for PCOS, meaning that dysfunction in the brain, specifically in the hypothalamus, is the main cause of ovarian androgen excess. It works like this:
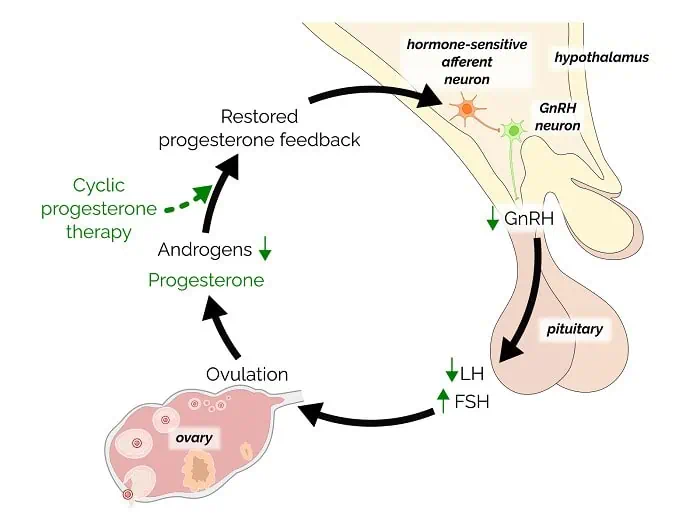
In a normal, healthy menstrual cycle, the hypothalamus releases pulses of GnRH (gonadotropin-releasing hormone), first slowly, then more rapidly, and then slowly again after ovulation. In turn, those pulses stimulate pituitary hormones (FSH and LH) that coordinate ovulation and promote the healthy production of estrogen and progesterone.
A key feature of a healthy neuroendocrine system is progesterone’s beneficial slowing effect on GnRH pulsatility. In other words, progesterone (made by ovulation) exerts beneficial negative feedback on the hypothalamus, lowering androgens and promoting future ovulation.
With PCOS, rapid GnRH pulses result in chronically elevated LH, androgen excess, insulin resistance, and, ultimately, progesterone deficiency due to anovulation.
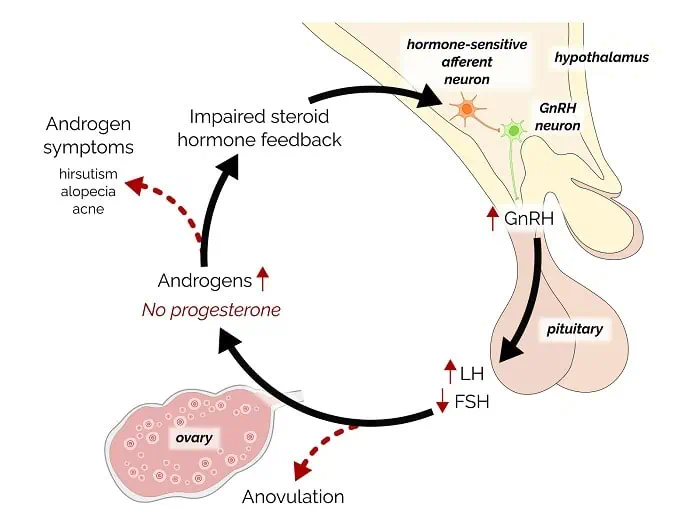
Unfortunately, progesterone deficiency then promotes a vicious cycle of impaired feedback on the hypothalamus, leading to persistently rapid GnRH pulses and further anovulation.
👉🏽 Tip: High GnRH pulsatility is ultimately caused by a combination of genetics and epigenetics resulting from in-utero exposure to androgens and environmental toxins. High insulin or insulin resistance also contributes to high GnRH pulsatility.
Cyclic progesterone therapy to lower androgens
According to Professor Jerilynn Prior, “cyclic progesterone therapy is treatment with the natural progesterone hormone (oral micronized progesterone, Prometrium® or compounded in oil) in a way that mimics the normal pattern (14 days in the last half of the menstrual cycle) and amount (300 mg at bedtime).”
In our paper, Professor Prior and I explore three main mechanisms by which cyclic progesterone therapy can improve androgenic PCOS:
- By regulating the hypothalamus, cyclic progesterone therapy can lower LH and restore normal ovulation.
- By lowering DHT, the active form of testosterone. It does this by competing with the enzyme 5-alpha-reductase—the same enzyme that converts progesterone to the calming neurosteroid allopregnanolone.
- By increasing metabolic rate and lowering androgens. That’s why progesterone can promote weight loss and improve insulin resistance.
How to take cyclic progesterone therapy
Many of my PCOS patients have had success with cyclic progesterone at a lower dose of 100 mg at bedtime. Taken cyclically, two weeks on, two weeks off.
💡Tip: It’s best to take progesterone at bedtime because oral progesterone can be very sedating. Taking it during the day can cause grogginess and depression.
If cycles are irregular and anovulatory, the starting dose is two weeks on and two weeks off until regular ovulation can be established. (The initial bleeds induced by progesterone are withdrawal bleeds, not ovulatory cycles. And if cyclic progesterone does not induce a withdrawal bleed, it might not be PCOS.)
Once cycles become ovulatory, switch to taking progesterone only during the two weeks of the luteal phase (i.e. starting a day or two after ovulation). After six or more ovulatory cycles, you may be able to stop taking progesterone because you’re now making it.
To obtain oral micronised progesterone, you’ll need a prescription from your doctor. You could try saying:
“Could I please try a few months of Prometrium for PCOS? According to this Canadian endocrinology professor, progesterone can induce a withdrawal bleed and improve androgen symptoms.”
Show your doctor a printed copy of our paper and point out that, in terms of breast cancer risk, progesterone is safer than a progestin. If your doctor is hesitant, offer to leave it with her and return for a second appointment. (Email me for a PDF copy of the full paper.)
Is progesterone safe?
Unlike progestins, which can increase the risk of breast cancer, body-identical progesterone is safe. For example, progesterone is usually beneficial for mood and sleep, and according to Professor Prior, natural progesterone may even help to reduce the risk of breast cancer.
Progesterone is also usually better for mood than a progestin, but some women are sensitive. Read Troubleshooting progesterone.
As discussed in my Guide to progesteroneblog post, cyclic progesterone therapy can also treat perimenopause, heavy periods, endometriosis, adenomyosis, migraines, and premenstrual mood symptoms, including PMDD.
In conclusion, cyclic progesterone therapy is potentially beneficial for PCOS. It can be safely combined with other PCOS treatments, such as metformin, spironolactone, and inositol. Ask me in the comments.